Chronic lower back pain is persistent pain in the lower back that lasts more than 12 weeks. It is complex and not just a structural issue. It also involves pain sensitivity, deconditioning, and movement avoidance patterns.
Does exercise help with it? To no surprsise, the answer is yes…but perhaps not in the way many people think.
A recent Cochrane systematic review (highest quality evidence out there) by Hayden et al. examined the effectiveness of exercise for chronic non-specific low back pain. The review included hundreds of randomized controlled trials involving thousands of participants, making it one of the most comprehensive analyses available on the topic.
Here is what they found:
Exercise Works
Compared to no treatment, placebo interventions, or usual care, exercise produced meaningful improvements in pain and modest improvements in function.
Pain improved by approximately 15 points on a 100-point scale.
Functional ability also improved, although the average change was smaller.
Overall, exercise was found to be an effective treatment for chronic low back pain.
Importantly, these benefits were seen across a wide variety of exercise approaches rather than being limited to one specific method.
Is One Type of Exercise Best?
This is where the findings become particularly interesting.
The review found that most exercise approaches appear to be effective, including:
Strength training
Aerobic exercise
Motor control exercises
Yoga
Pilates
McKenzie exercises (repeated postures that are suspected to improve your pain- i.e. extensions with disc injuries)
Flexibility programs
Multimodal exercise programs
While some previous analyses suggested that Pilates, McKenzie-based exercise, and functional restoration programs may provide slightly greater improvements in pain and disability, the differences between exercise types were generally small.
In other words, no single exercise approach consistently outperformed all others. Not sure exactly what to do? Just get active and figure it out as you go!
Specific Exercises vs General Exercise
One of the biggest takeaways from the review is that the benefits of exercise may be less about the exact exercises performed and more about simply becoming active and progressively increasing movement capacity.
This challenges the common belief that patients must find the “perfect” exercise program to recover. While exercise selection still matters, the evidence suggests that many different approaches can be successful when they are performed consistently and progressed appropriately.
The review supports a more flexible approach where exercise can be tailored to the patient’s preferences, goals, physical abilities, and symptom presentation rather than forcing everyone into the same program.
Why Does Exercise Help?
Exercise likely works through multiple mechanisms.
Physical benefits may include:
Increased strength and endurance
Improved movement tolerance
Better spinal and whole-body conditioning
Progessively challenging tissues to handle load again
Psychological and neurological benefits may include:
Reduced fear of movement
Increased confidence in the back
Improved self-efficacy
Positive effects on pain processing
This may help explain why many different exercise approaches can produce similar outcomes.
Is Exercise Safe?
The review found that exercise is generally very safe for people with chronic low back pain.
Reported adverse events were uncommon and were usually limited to:
Temporary increases in soreness
Mild increases in back pain
Exercise-related discomfort
Serious adverse events were rarely reported.
Practical Applications
For clinicians and patients, the message is fairly straightforward:
Exercise should be considered a first-line treatment for chronic low back pain.
Most exercise approaches are likely beneficial.
No single exercise method has proven to be universally superior.
Consistency and long-term adherence appear to be more important than finding the perfect exercise.
Programs should be individualized based on patient goals, preferences, and physical capacity.
Bottom Line
Exercise is one of the most effective non-pharmacological treatments for chronic low back pain. While certain approaches such as Pilates, McKenzie therapy, and functional restoration programs may have slight advantages, the overall evidence suggests that most forms of exercise can help.
One key thing is it’s hard to get super specific with a diagosis in a large scale study, so the specificty of a plan tailored to your injury might be more worthwhile than this review shows
That being said, the best exercise program is often not the most specialized program. Really what you want to look for is the plan that you are willing to do, and will enjoy doing consistently over a long period of time.
Chose something specific to your injury if that overlaps with what you are willing and want to do, but more than anything, go with the plan that you enjoy the most! Keep moving regularly. Build tolerance to load over time. Be patient, and good things will happen!
If you want to review how to implement exercise into your low back pain managemnet program- feel free to contact or book with one of our Waterloo based chiropractors, physiotherapists or RMTs HERE.
Exercise significantly increased lumbar spine BMD in women under 30
Exercise significantly increased femoral neck BMD in women under 30
Effect sizes were moderate
Lumbar spine: SMD ~0.46
Femoral neck: SMD ~0.42
Beyond these primary findings, the review showed that the type of exercise performed plays an important role in determining outcomes.
Programs that combined resistance training with weight-bearing or impact activities consistently produced the largest improvements in bone density.
These combined approaches appear to create a stronger mechanical stimulus by loading bone in multiple ways, which enhances adaptation.
In contrast, single-mode exercise such as endurance or aerobic training alone resulted in smaller or less consistent changes in BMD. This reinforces the idea that bone responds best to varied and progressively challenging loading rather than repetitive, low-variation activity.
Bone Turnover Markers
The study also examined changes in bone turnover markers, which provide insight into how bone is actively remodeling. Exercise increased markers of bone formation, including osteocalcin and bone-specific alkaline phosphatase, indicating that bone-building processes were being stimulated. Shorter training programs, particularly those under four months, were associated with early increases in markers like osteocalcin and P1NP, suggesting that biological changes in bone can occur relatively quickly, even before large changes in density are measurable. Bone-specific alkaline phosphatase increased with both short- and longer-term training, supporting the idea that continued exercise helps maintain this positive remodeling environment.
Start Young!
One of the more notable findings relates to age.
The review found significant improvements in bone density in women under 30, but not in those over 30.
At first glance, this may suggest that exercise becomes ineffective for bone health after early adulthood, but that interpretation would be misleading. Bone tissue is most responsive during the years leading up to peak bone mass, which typically occurs in the late twenties. After this point, the body becomes less sensitive to mechanical loading, meaning it is harder to produce measurable increases in bone density over shorter study periods.
However, this does not mean exercise is no longer beneficial for women over 30. In this group, exercise still plays a critical role in maintaining existing bone mass and slowing age-related decline. Without regular loading, bone density tends to decrease gradually over time, increasing the risk of osteoporosis later in life. Exercise, particularly resistance and impact training, helps preserve bone structure, improve strength, and reduce fracture risk even if large increases in BMD are not seen.
In other words, while younger individuals may be building bone, older individuals are protecting what they have, which is just as important!
Practical Applications
Exercise can improve bone density in young adult women, but not all exercise is equally effective.
Programs that combine resistance training with weight-bearing or impact activities produce the best results.
The largest gains are seen before the age of 30- put as much bone density in the bone bank as possible during your younger years!
Exercise remains highly valuable afterward by helping maintain bone mass and reduce long-term risk. If you’re over 30, don’t stress about what you may or may not have done in your younger years- work to maintain what you have with resistance training mixed with some impact -oriented cardiovascular exercise!
If you have any questions about how to structure a program to maintain bone density- feel free to contact our Waterloo based chiropractors, physiotherapists or book online HERE.
Glucosamine is a naturally occurring amino sugar that is found in the human body and is involved in the formation and repair of cartilage, particularly within joints. As a supplement, it is most commonly used by individuals with osteoarthritis in the hope that it can slow cartilage breakdown, improve joint function, and reduce pain. It is often sold as glucosamine sulfate or glucosamine hydrochloride, sometimes combined with chondroitin sulfate, another compound found in cartilage.
How is glucosamine thought to work (theoretical mechanism)?
The proposed mechanisms (mostly based on laboratory and animal studies, not strong human evidence) include:
Serving as a building block for glycosaminoglycans, which are components of cartilage
Potentially stimulating cartilage repair or slowing breakdown
Possible anti-inflammatory effects within the joint
Reducing activity of enzymes that degrade cartilage (e.g., matrix metalloproteinases)
However, it is important to note that these mechanisms are largely theoretical in humans, and the clinical effect in real-world trials has been uncertain.
Study
The GAIT (Glucosamine/Chondroitin Arthritis Intervention Trial) was a large, high-quality clinical trial funded by the U.S. National Institutes of Health (NIH). It was designed to rigorously test whether glucosamine, chondroitin sulfate, or their combination could reduce pain and improve function in patients with knee osteoarthritis. It is considered the gold standard study on this topic!
Total participants: 1,583 patients with knee osteoarthritis
Duration: 24 weeks
Treatment groups:
Glucosamine hydrochloride (1500 mg/day)
Chondroitin sulfate (1200 mg/day)
Combination of both
Celecoxib (NSAID active control)
Placebo
Primary outcome: ≥20% reduction in knee pain
The inclusion of celecoxib was important because it acted as a benchmark to confirm the trial could detect real treatment effects if they existed.
Results:
Primary outcomes
No statistically significant difference between placebo and:
Glucosamine alone
Chondroitin alone
Glucosamine + chondroitin
Active control
Celecoxib showed a clear and statistically significant reduction in pain compared to placebo
This confirmed the study design was sensitive enough to detect true analgesic effects
In other words- it glucosamine + chondroitin was going to work, the study would have shown it!
Subgroup analysis
In patients with moderate-to-severe baseline pain:
Combination glucosamine + chondroitin showed a higher response rate than placebo
This effect was:
Not consistent across all analyses
Considered hypothesis worth studying more, but definitely not definitive
Secondary outcomes
No meaningful or consistent improvement in:
Physical function
Joint stiffness
Overall osteoarthritis symptom scores
Safety outcomes
Glucosamine and chondroitin were generally:
Well tolerated
Similar adverse event rates compared to placebo
No major safety concerns identified
Practical Applications
In the end, this study showed that despite biologically plausible mechanisms, glucosamine (with or without chondroitin) did not provide meaningful clinical benefit for most patients with knee osteoarthritis.
While there was a possible signal of benefit in a subgroup with more severe pain, this was not strong or consistent enough to change overall conclusions. Celecoxib’s positive results supported the validity of the trial design, strengthening confidence in the negative findings for glucosamine.
In the end it’s safe to try glucosamine, but go in knowing that you will likely not see any change, and if you do notice a change, it’s very likely identical to what a placebo would provide.
There’s nothing worse than hearing you have a stress fracture as a runner (maybe)! This 2024 review of systematic review will help to arm you with the information you need to avoid them and catch them early!
What This Study Is About Stress fractures are overuse injuries that develop when repeated mechanical loading exceeds the bone’s ability to recover. The paper explores how frequently these injuries occur, where they are most likely to happen, what contributes to their development, and how they are best diagnosed and treated.
How the Research Was Done The authors reviewed evidence from major databases – primarily systematic reviews. Around 90 studies were initially identified, with approximately 57 included in the final analysis. This is the best of the best!
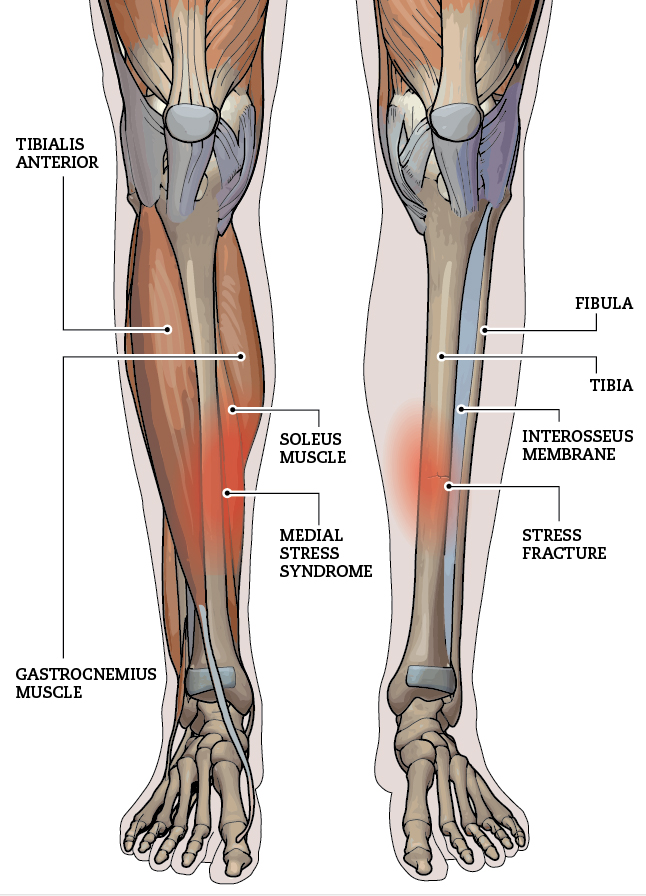
Where Stress Fractures Happen Most Stress fractures occur predominantly in the lower extremities due to repetitive loading during running. In long-distance runners, the tibia is the most commonly affected bone, followed by the metatarsals. In contrast, sprinters tend to experience more stress fractures in the toe bones, likely due to the higher forces and forefoot loading associated with sprinting mechanics.
Why Stress Fractures Develop Stress fractures are multifactorial and typically result from a combination of biological, nutritional, mechanical, and psychological factors.
Key factors include:
female sex
reduced bone density
nutritional factors such as low energy availability and deficiencies in calcium or vitamin
Training-related issues, particularly rapid increases in workload
In addition, psychological factors like high stress levels, perfectionism, and fear of failure may indirectly increase injury risk by influencing training behaviours and recovery.
How They Are Diagnosed Diagnosis begins with a detailed clinical history and physical examination, but imaging is often required for confirmation.
MRI is considered the most sensitive and preferred method for detecting stress fractures, especially in the early stages.
X-rays are commonly used but may not detect early bone stress injuries, which can delay diagnosis if relied upon alone.
Bone scans are the fastest and most sensitive option for most of us in Canada.
What Treatment Looks Like Treatment primarily involves reducing or temporarily stopping the activity that caused the injury, allowing the bone time to heal. A gradual return to running is introduced once symptoms improve. Importantly, treatment should also address the underlying factors that contributed to the injury- see above!
How to Reduce Your Risk Preventing stress fractures requires a proactive approach that includes maintaining adequate nutrition and energy availability, progressing training loads gradually, and addressing any biomechanical inefficiencies. Screening for conditions such as RED-S or the Female Athlete Triad may also be important in certain populations. Psychological stress should not be overlooked, as it can influence both training habits and recovery- are you doing the right thing for your training, or are you responding to anxiety that is telling you to illogically ramp up?
Practical applications:
Most stress fractures occur in the lower extremities
Tibia is the most common site in long-distance runners
Metatarsals are the second most common
Sprinters more commonly experience stress fractures in the toes
Risk factors include biological, nutritional, mechanical, and psychological components
MRI is the most sensitive diagnostic tool, bone scan is probably our best choice in Canada
Treatment focuses on rest, gradual return, and addressing underlying causes
Prevention requires proper training progression, nutrition, and overall load management
Managing anxiety related to training and racing is a huge factor for most competitive runners!
If you have any questions about any of your injures for our Waterloo based chiropractors, physios or RMTs- feel free to contact us or book online HERE.
Tibial stress fractures (TSFs) are common overuse injuries in runners. They happen when repeated force on the shinbone causes tiny cracks that outpace the body’s ability to repair them. Many clinicians and coaches think that the way someone runs – their biomechanics – might influence who gets these injuries. This 2023 review study set out to find out whether runners with TSFs really move differently from runners without them.
How Did They Study It?
The authors searched major research databases for studies that compared running mechanics between injured runners and healthy controls. They found 359 possible papers, but only 14 met strict criteria for analysis. Most of these studies were retrospective (looking back at runners after injury) and had small sample sizes- so as always, more research that prospective and more controlled would be nice!
What Did They Find?
When all the data were combined:
There were no significant differences in ground reaction forces between runners with TSFs and uninjured runners. In other words, impact and braking forces were similar in both groups.
Some individual studies did find differences in variables like tibial stress, tibial acceleration, rearfoot motion, or hip movement, but these findings were not consistent across studies.
What Does This Mean?
Based on the best available evidence:
We can’t confidently say that runners with tibial stress fractures have a distinct running biomechanics profile.
Current studies are too small and too varied to draw strong conclusions.
Larger, better‑designed research is needed to clarify whether specific movement patterns truly increase the risk of TSFs.
In the meantime- stick with the things we KNOW related to printing stress fractures:
Adequate caloric intake
Vitamin D supplementation
Adequate calcium intake
Strength work
Being smart with your training load- building slowly, taking recovery days and weeks strategically
If you have any questions about pain you’ve been feeling- feel free to contact our Waterloo based chiropractors, physiotherapists or book online HERE.
Anybody who has had plantar fasciitis knows how annoying and painful it can be. A common treatment we see out there is the use of therapeutic ultrasound- but does it actually help? That’s what this 2025 meta analysis looked at.
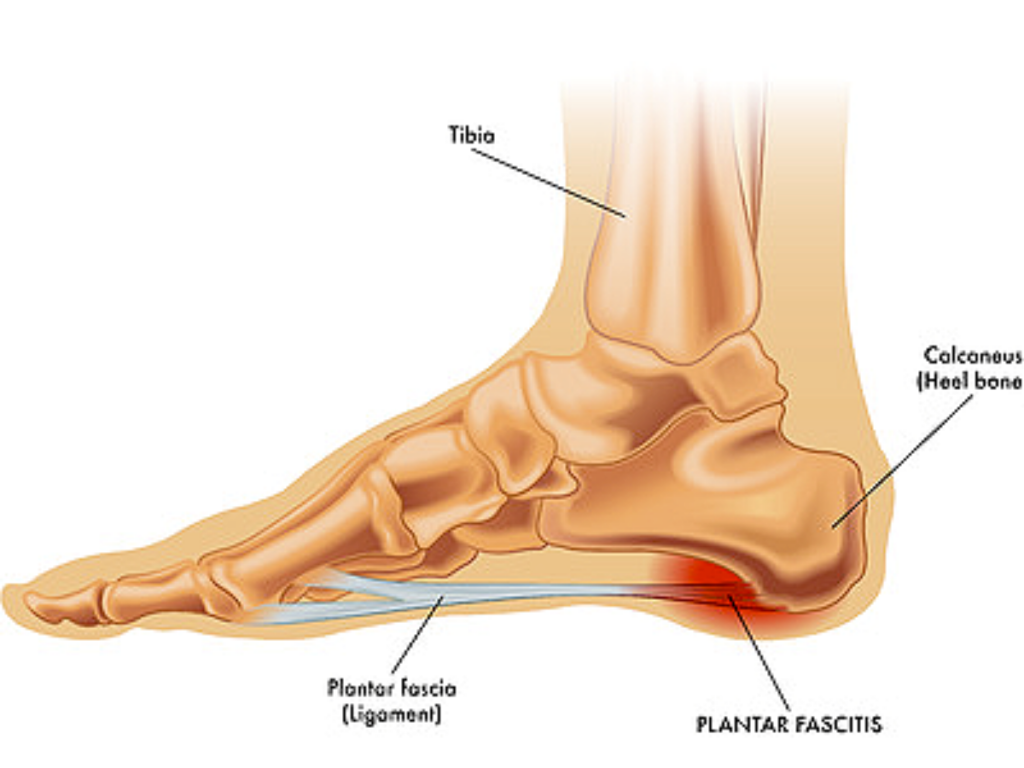
Plantar fasciitis is a common cause of heel pain that is often associated with overuse, repetitive loading, and biomechanical factors. The attachment at the heal biomes irritated, and the pain can sometimes be debilitating – especially in the mornings!
The authors performed a meta-analysis of 13 clinical trials including 594 participants. The main outcomes of interest were pain intensity and foot function. Pain was measured using visual analog and numeric pain scales, while function was assessed using the Foot Function Index (FFI) and the American Orthopaedic Foot and Ankle Society (AOFAS) score.
Key Findings
Pain intensity
Ultrasound alone did not show a statistically significant improvement in pain compared with no treatment.
Adding ultrasound to conventional physical exercise programs did not provide additional pain relief compared with exercise alone.
When ultrasound plus exercise was compared with other interventions combined with exercise, some statistically significant differences were observed, but these generally favoured the other treatment groups.
In general, the authors concluded that ultrasound is not reliable as a primary modality for reducing plantar fasciitis pain.
Foot function
Ultrasound combined with exercise may provide small improvements in foot function when measured using the Foot Function Index.
Results were inconsistent across functional outcome measures.
There was no statistically significant difference in AOFAS scores between treatment groups in some analyses.
Mechanism of Action Discussion
The authors discussed potential biological effects of ultrasound therapy. Ultrasound may promote tissue healing through both thermal and non-thermal mechanisms. Thermal effects may improve local blood circulation, while non-thermal effects such as cavitation and micromassage may influence cellular activity and inflammation.
However, the heat generated by therapeutic ultrasound may not be sufficient to produce meaningful clinical effects in plantar fascia tissue over short treatment periods. Low-intensity pulsed ultrasound has been studied in other conditions and may have anti-inflammatory and tissue repair effects, but evidence in plantar fasciitis remains limited.
Plus- how much better is any of this than just applying a heating pad and loading the tissue with exercise?
Limitations
As with most research for muscle and joint pain, more research is always needed!
Only 13 studies were included, and high-quality randomized controlled trials were limited.
There was significant variation in ultrasound treatment parameters such as frequency, intensity, and treatment duration.
Many of the trials were many years (and decades) old!
Practical Applications
Therapeutic ultrasound, whether used alone or combined with conventional exercise programs, does not appear to provide meaningful pain reduction in plantar fasciitis. Ultrasound may have a small positive effect on foot function, but the clinical significance of this finding is uncertain. More high-quality randomized trials are needed…but if I had to bet, it’s likely just a waste of time trying it when strengthening and progressive loading is so much more effective and important!
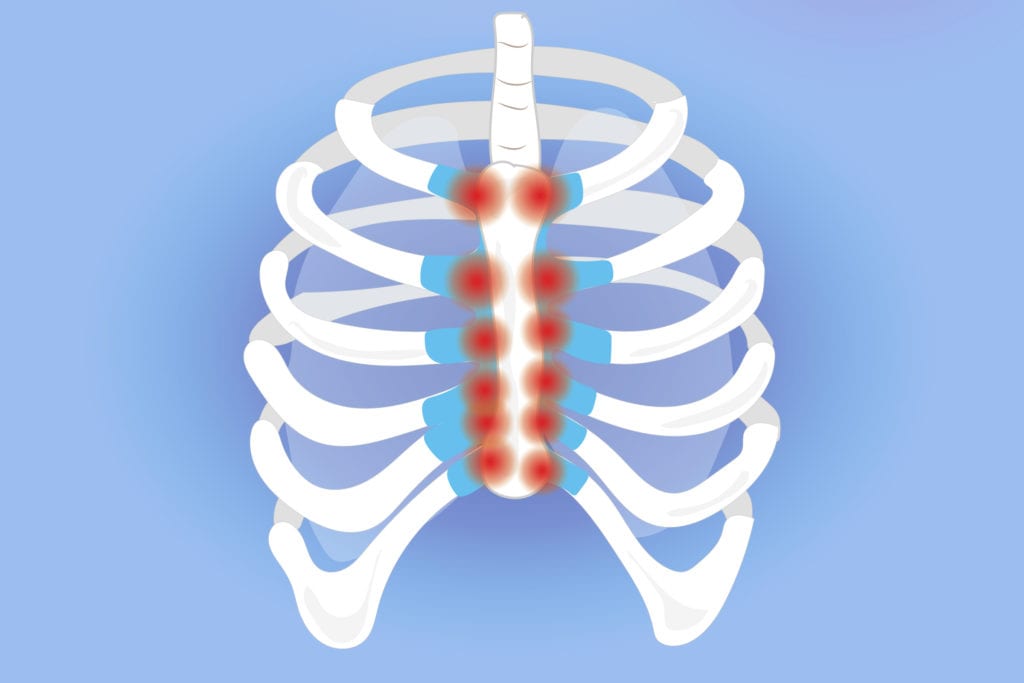
What is costochondritis? Costochondritis is inflammation of the cartilage where the ribs attach to the sternum. It causes localized chest wall pain that can mimic heart-related pain but is not caused by cardiac disease. This summarytakes an in-depth look at the most up to date research regarding this condition.
It is considered one of the more common musculoskeletal causes of chest pain and may account for up to about 30 percent of noncardiac chest pain cases seen in some clinical settings.
Clinical presentation -Pain is usually localized and reproducible with palpation over the affected costosternal or costochondral joints. -The pain may be sharp or aching. – Symptoms often worsen with movement, deep breathing, or pressure on the chest wall. – There is usually no visible swelling, redness, or systemic symptoms such as fever.
Diagnosis – There is no specific laboratory test or imaging study that confirms costochondritis. – Diagnosis is clinical and based primarily on history and physical examination. – A key diagnostic feature is reproduction of pain with palpation of the anterior chest wall. – Cardiac and other serious causes must first be excluded, especially in higher-risk patients.
Management – Initial treatment is conservative and may include: Analgesics such as acetaminophen and Nonsteroidal anti-inflammatory drugs (talk do your doctor!) – Relative rest and activity modification is key. Complete rest isn’t good, but continuing with the activities that aggravate the condition do not allow for it heal!
Physiotherapy is also a crucial part of the management of this condition. Some examples include:
Stretching and mobility exercises These focus on improving chest wall and thoracic spine mobility.
Examples include: Pectoral stretching, such as doorway stretches Thoracic extension and mobility exercises Breathing-based mobility drills to reduce rib cage stiffness
Manual therapy
Performed by trained clinicians, this may include:
Soft tissue mobilization of the chest wall and surrounding musculature
Joint mobilization of the ribs and thoracic spine
Trigger point release and myofascial techniques
Rib mobilization techniques to normalize movement
Some small clinical studies and case series suggest that combining manual therapy with therapeutic exercise can reduce pain and improve function the most, but as always more research is needed!
Main takeaway Costochondritis is an important and relatively common cause of noncardiac chest pain. It is diagnosed clinically after ruling out more serious co
nditions. Management is usually conservative and may include medication, rest, and targeted physical therapy interventions aimed at improving chest wall mobility, posture, and muscle function.
If you have questions about your pain, feel free to contact one of our Waterloo based chiropractors or physiotherapists, or book online HERE.
I’ve written about it before, but it’s time for another update! Sure, running can be linked to short and moderate term problems like tendonitis, but what about longterm wearing out of your joints even if you do everything right? That’s what THIS 2023 systematic review looked at.
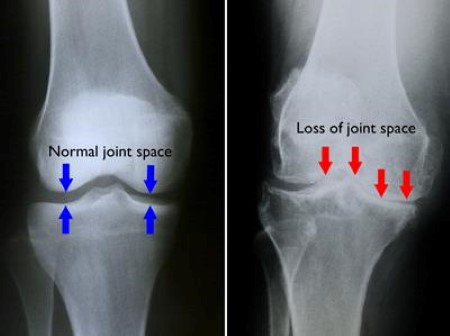
The Study This study is a systematic review, meaning the authors collected, analyzed and combined results from many of the previous highest quality studies looking at runners and non-runners to see whether running affects the development of knee osteoarthritis (OA). The review included 17 studies with over 14,000 participants. Knee health was assessed using imaging (such as X-rays or MRI) and patient-reported outcomes like pain and function.
Key results: – Knee pain was reported more often in non-runners than in runners. – Most studies found no meaningful differences in structural knee osteoarthritis (such as joint space narrowing or OA severity on imaging) between runners and non-runners. – One study reported more bone spurs (osteophytes) in runners, but this finding was not consistent across other studies. – Some evidence suggested that non-runners had a higher risk of needing knee replacement surgery than runners.
Practical Applications:
Our bodies are meant to move! This review shows that running does not appear to increase the risk of developing knee osteoarthritis. Running was not associated with worse imaging findings and may be linked to less overall knee pain compared to not running.
That doesn’t mean runners will not develop OA, but it does mean that odds are running is not to blame if it does. It also shows that there’s a chance that running helps to reduce general pain and reduce the odds of needing replacement down the road.
There are obviously many caveats to this- such as if you currently have severe OA it’s probably not a good time to start running. Talk to your health practitioner about of this research applies to you. However, what this review does tell us is the blanket statement of “running wears out knees” simply isn’t true!
It can be a scary thing when you rupture your Achilles tendon! Yes recovery can be a long process, but virtually full recovery is possible in many case. The interesting thing that many don’t realize however is that OFTEN rehab is just as good as surgery– which is something this 2019 review study looked at.
Objective
The aim of this systematic review and meta-analysis was to compare operative and nonoperative treatments for acute Achilles tendon rupture. The authors focused on differences in tendon re-rupture rates, complication rates, return to work, and functional recovery between treatment approaches.
Study Design
The authors searched several medical databases to identify randomized controlled trials comparing surgical and nonoperative management of acute Achilles tendon rupture.
Fourteen randomized controlled trials were included, representing a total of 1,628 patients.
The average follow-up period across studies ranged from 6 months to over 2 years.
Outcomes analyzed included re-rupture rates, overall complication rates, Achilles Tendon Total Rupture Score (ATRS), ankle range of motion, and time to return to work.
This was a well designed study!
Results
• The overall re-rupture rate was significantly lower in the open surgical group compared to the nonoperative group, with re-rupture occurring in approximately 1 to 3 percent of surgically treated patients versus about 6 to 12 percent of nonoperatively treated patients. • Minimally invasive surgical repair also showed a lower re-rupture rate than nonoperative treatment, with re-rupture rates closer to those seen with open surgery. • Open surgical repair was associated with a higher rate of complications, with overall complication rates reported between 10 and 20 percent, including wound infection, delayed healing, and nerve injury. • Nonoperative treatment showed lower rates of these surgical complications, generally below 5 percent. • Minimally invasive surgery demonstrated complication rates similar to nonoperative treatment and lower than open surgery. • Functional outcomes, including ATRS scores, showed no statistically significant difference between operative and nonoperative groups at final follow-up, with most studies reporting ATRS scores in the range of 80 to 90 points for both groups. • Measures of ankle range of motion and calf strength were also similar between groups. • Patients treated with minimally invasive surgery returned to work earlier, on average 1 to 3 weeks sooner, compared to those treated nonoperatively.
How does this apply to you?
This review found that surgical treatment of acute Achilles tendon rupture reduces the risk of tendon re-rupture compared with nonoperative management but increases the risk of complications, particularly with open surgery. Minimally invasive surgical techniques appear to balance lower re-rupture rates with fewer complications and may allow an earlier return to work.
That being said, long-term functional outcomes were similar between surgical and nonoperative treatments, suggesting that both approaches can lead to comparable recovery when appropriate rehabilitation is provided.
So this isn’t a one-option fits all treatment. Do you have a daily life that puts you at risk for re-rupture? Do you have a less active/ risky lifestyle with a high need to get back to work ASAP? These are the types of questions you want to ask yourself when making the choice that’s right for you.
If you have more questions or you want to book with one of our physiotherapists based in Waterloo, you can do so HERE.